BRUCKER
METHOD
1) Introduction
2) How It Works
3) Biofeedback for SCI
4) Questions and Answers
5) Conclusion
6) Availability
INTENTION
CONTROLLED MYOFEEDBACK (IMF®)
Introduction:
Biofeedback is a subtle training technique used to enhance mind-body
control. By providing subjects with external audio or visual feedback of
subtle nervous signals that reach the muscles, using electrodes to sense
the signals, biofeedback provides a means for identifying, strengthening,
and using these signals. Through this technology, biofeedback lets
subjects know when they are changing their physical responses – such as
nerve signal strength, body temperature, blood pressure, or heart rate –
in desired directions. This information can be used to teach individuals
to better control their body.
Under certain
conditions, biofeedback can assist individuals with SCI to regain or
improve functional usage of motor nerve cells in the brain, brain stem,
and spinal cord, which can lead to improved use of disabled limbs.
Dr. Bernard
Brucker, Founder of the Biofeedback Laboratory at the
University of Miami’s School of Medicine, developed an internationally
recognized biofeedback method that uses precise techniques to restore lost functions in those with
neural impairment, called the Brucker Method. According to Brucker, his
aim in developing his method was to improve the lives of those with
neurological motor impairment by providing a bridge between neuroscience
and rehabilitation.
that uses precise techniques to restore lost functions in those with
neural impairment, called the Brucker Method. According to Brucker, his
aim in developing his method was to improve the lives of those with
neurological motor impairment by providing a bridge between neuroscience
and rehabilitation.
Biofeedback was
initially viewed with skepticism by traditional medicine. However,
repeated studies confirmed that individuals could change both voluntary
and involuntary responses after being fed back information that revealed
what was occurring in their bodies. After treatments, patients retain the
ability to repeat learned responses at will, without visual or audio
feedback.
In 1969, the
use of audio-visual information to train subjects to alter blood pressure,
heart rate, muscle tension, and brain activity was first termed
“biofeedback.” O. Hobart Mowrer pioneered the use of instruments to
control bodily functions in 1939, using alarms triggered by urine to stop
children from bedwetting. Biofeedback first gained the public’s attention
in the late sixties, when it was used to demonstrate the biophysical
self-control of yogis in altered mental states.
Biofeedback
has been used to treat migraine headaches, tension headaches, chronic
pain, digestive-system disorders, urinary incontinence, high blood
pressure, cardiac arrhythmias, attention deficit hyperactive disorder,
Raynaud’s disease, epilepsy, SCI, stroke, traumatic brain injury, cerebral
palsy, and various movement disorders.
How Biofeedback Works
“A reinforcing stimulus is roughly the same as a reward. If a person does
something and receives a ‘reinforcer,’ he will probably do the same thing
again the next chance he gets.” —Richard Malott, (1972)
Biofeedback is
a form of operant learning; psychologist
Leland Swenson says of EMG biofeedback as an operant training technique:
EMG biofeedback has been extended into the medical areas of deficient
neuromuscular control. Inglis, Campbell, and Donald (1976) reviewed
applications of EMG biofeedback in treating peripheral nerve muscle
damage, the effects of strokes, partial paralyses, and cerebral palsy
(early brain damage having a motor component). They cite considerable
evidence to suggest that patients can learn to gain more control over the
involuntary activity of voluntary muscles. This neuromuscular reeducation
approach has been successful in restoring function to paralyzed limbs
where some neural control remains. Within a couple of hours, those
patients who had at least a few intact nerve endings were producing
sufficient motor unit action potentials from these surviving nerve endings
to achieve large percentages of normal, voluntary muscle functioning. The
various studies reported 50% to over 85% of patients benefited from such
treatments. [Applications
of Operant-Related Learning Principles to the Real World, Leland
Swenson]
For SCI
applications, the Brucker method of biofeedback operant training uses
electromyography (EMG), which senses motor action potentials (nerve
“impulses” or signals) with far greater precision and sensitivity than the
user can. Electromyography therapy determines the bioelectrical function
of a patient's muscles, which indirectly reveals the functional condition
of the spinal cord and brain.
During
biofeedback treatment, the patient is requested to perform intended
movements. Using a movable graph on a computer screen, EMG provides visual
feedback of neural signals that reach the target muscles. The subject may
need repeated attempts to “find” a neural pathway that delivers a signal
to target muscles. But even then the signal is often too weak for the
subject to sense.
Once a neural
path is found, the therapist directs the subject to make the EMG graph
“grow.” This can only occur by increasing the strength of the motor signal
that reaches the muscle. However, because the subject may not sense the
signal, or signal variations may be too slight to be felt at first, the
moving chart provides the reinforced stimulus necessary for operant
learning to occur.
Thus, visual
feedback teaches the subject how to reproduce, maintain, and control EMG
responses for maximum improvement in muscle function. This information,
combined with behavioral conditioning techniques and rehabilitation, helps
subjects reeducate their muscles. The level of control gained in one
session is the starting point for the next.
Biofeedback for SCI:
For SCI, the Brucker Biofeedback Technique uses the Neuroeducator 3
Electromyography (EMG) Biofeedback System, which allows therapists to
identity subtle motor connections between the brain and the body that
survive SCI, or that have slowly repaired or rebuilt since being damaged.
This information allows therapists to design individually customized plans
aimed at restoring or improving voluntary muscle control.
The Brucker
technique is the only biofeedback protocol specifically designed to
enhance neural conduction and functions in subjects with neurological
injury and disease. Unlike general uses of biofeedback to enhance
relaxation, or to control blood pressure or heart rate, biofeedback for
SCI requires equipment sensitive enough to monitor neural signals to
within one percent of a normal signal. In addition, for SCI applications
biofeedback-trained therapists should know which muscles are needed to
regain specific motor functions, the signal strength needed for specific
muscles to function, and techniques for helping the subject find and
develop these signals.
People with SCI
have regained much lost motor function after biofeedback training. The
results sometimes appear as miraculous. People who were told that they
would never walk or use their hands have regained the ability to walk or
feed themselves. Restored functions become natural through practical use.
However, motor improvements through biofeedback training require specific
physical conditions:
1.
A neural connection must exist between the brain and the muscle (or
muscle group) that is desired to move. Such connections might have
survived initial SCI, or they may have repaired over time, or they may be
the spinal cord’s attempt to rewire itself through existing connections.
2.
The patient must be aware and able to mentally respond to therapist
directions.
3.
Muscular atrophy or contractures cannot be so severe that they’re
unable to be corrected. Electrical stimulation therapy may be needed to
strengthen or rebuild atrophied tissues, allowing them to fully benefit
from biofeedback. Because physiatrists can be reluctant to prescribe such
therapy to retard or reverse atrophy when no obvious muscle contractions
are present, biofeedback evidence of an existing signal can be used to
show a need.
4.
Biofeedback can be used to monitor any neural signal provided that
an external electrode can be positioned to sense and relay the signal to
an external device that’s able to represent the signal’s presence and
strength. Although biofeedback can be used to improve functions in the
hands or feet, muscles in fingers or toes can be too small for electrodes
to fit.
Understanding
biofeedback potentials and limitations reveals the importance of
maintaining muscle tone, flexibility, and bone density through personal
care. The above requirements are needed not only in using biofeedback to
train the body in using existing, but disused neural connections, but will
also be needed for individuals with SCI to benefit from emerging
treatments that repair or regenerate the spinal cord.
Sources of
neural connections through the spinal cord after SCI include, for example,
existing pathways, alternate pathways, damaged pathways that spontaneously
repair over time, pathways that spontaneously rewire over time, and
surgically reconstructed pathways
According to
Brucker, it is extremely rare that all of the cord’s neural connections
are lost due to SCI. A “complete” classification of SCI (compared to an
“incomplete” injury) is a functional description of neurological
symptoms, rather than a physical description of the spinal cord
itself. Nerve connections between the brain and muscles below the level of
injury often survive SCI, but signals over these connections are too weak
to be felt in a neurological examination or to move affected limbs.
In addition to
Brucker’s observations of biofeedback’s clinical use, studies involving
Transcranial Magnetic Stimulation provide supporting evidence. Dr. G.A.
Delaney and colleagues (London, Canada) found that axons could survive
through the injury site in patients with “longstanding” SCI, preserving "axonal
integrity in descending motor tracts in the face of extensive functional
loss."
Similar to the
brain, redundancy is believed to be part of the spinal cord’s design.
Several neural pathways may connect the brain to specific targets in the
body, rather than one. But a lifetime of repeated use conditions our
brains to see certain pathways as the connection for certain uses. Brucker
makes the analogy of a favorite route between the workplace and home. If
construction closes the road, we still go home – provided we find and
learn to use an alternate route.
Over time,
repairs may naturally occur to demyelinated axons, or broken axons may
find and remake lost connections in the injured spinal cord. Axon regrowth
is limited by the extent of gliosis (the formation of the “glial scar”
that occurs during acute SCI) and the presence of inhibitory molecules in
the spinal cord’s extracellular matrix, which were released due to damage
to myelin sheathing.
Finally,
medicine is beginning to test methods for repairing or regenerating the
damaged spinal cord. The brain may find it difficult to find and use newly
created neural connections, or repaired connections that have been
chronically “turned off.” For all these potentials, biofeedback provides a
means for finding, improving, and using these connections.
Biofeedback for SCI: Questions & Answers
1) How
does biofeedback work?
Biofeedback is
not a treatment in the sense that something is done to the subject.
Similar to learning to ride a bicycle, biofeedback teaches users to sense
and make use of potential abilities through experience. For
example, it’s impossible to explain the balance needed to ride a bicycle
to someone else. They need to feel it for themselves – but once felt and
controlled they retain the skill for life.
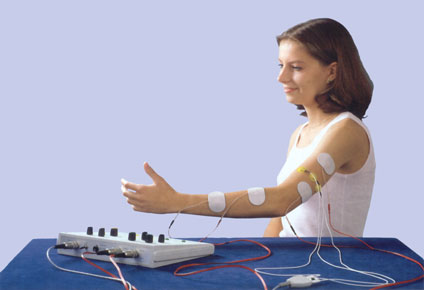
In practice,
biofeedback for SCI uses external electrodes to sense subtle neural
signals that reach the muscles when the subject tries to move them. The
electrodes relay this information to a device that’s able to represent the
signal and its strength visually, or with sound. The Brucker approach
usually presents a line graph that changes with increasing signal
strength.
Subjects are
directed to contract the monitored muscle. The EMG system is able to sense
and reveal slight neural signals that the subject may not feel. Once a
signal is found, the subject is instructed to try to focus not on the arm
or leg, but on the graph, while they attempt to make the graph grow. If
sounds are used, they’re instructed to turn the sound on or off. For
example, when attempting to decrease spasticity a subject may be directed
to turn a sound off, which would correspond to controlling the unwanted
‘spasticity’ signal. When directed to increase a motor signal the subject
would try to turn the sound on.
With
trial and error and repetition, subjects may find more effective pathways
for producing desired results. Once these pathways are found and used, the
brain remembers where they are and how to use them. Improvements gained in
one biofeedback session are the starting point for the next.
2) How
soon will the therapist know if improvements are possible?
A
biofeedback-trained therapist can tell during the first treatment whether
neural connections exist for each muscle tested. The likelihood of
functional improvements depends on the strength of motor signals that
reach the muscles. For example, the quadriceps requires roughly 14% of a
normal motor signal to trigger voluntary contractions. If 10% percent of a
normal signal reaches the muscle when the subject attempts to move it,
prior experience suggests that the movement threshold might be reached in
the first or second biofeedback session. More sessions are needed if the
initial signal is lower, but still strong enough to suggest that a
muscle’s functional threshold might be reached. If no signal can be found,
or if no improvement can be made on trace signals, it is unlikely that the
muscle’s functional threshold will be reached at that time. A
clinical study involving one hundred subjects with upper extremity SCI
reported the following:
“A significant increase in EMG
activity occurred from the triceps after one biofeedback treatment session
and further significant increases in EMG activity occurred after
additional biofeedback treatment sessions. Initial muscle strength and
initial EMG levels were not determining factors for response to the
biofeedback. The results suggest the efficacy of biofeedback for
increasing voluntary EMG responses in long term spinal cord injury
patients.”
3) Does
injury level or neurological “completeness” limit potential benefits?
Biofeedback therapy can lead to functional improvements in subjects with
SCI regardless of level of injury or completeness. Moreover, MRIs are
unable to accurately predict outcomes of biofeedback treatments, because
they are unable to determine the neural conductivity. Subjects with
injuries evaluated as “complete” have made substantial improvements
through biofeedback. Whereas others with slight to moderate incomplete SCI
have improved only slightly. According to Brucker, it is rare that
biofeedback therapy fails to exert some degree of positive effects.
4) Does
time post injury affect possible effects?
Biofeedback
treatment outcomes for those with SCI can be affected by time post injury
for the good or bad. Patients who had little neural sparing through
the injury site soon after injury can have considerable disused
connections ready to be found and used, once enough time elapses to permit
neural repair, or remodeling. On the down side, too much time post injury
contributes to muscle atrophy, contractures, and loss of bone density;
these can all adversely affect an individual’s ability to benefit from
biofeedback. For example, if a tendon becomes to too contracted, it may be
unable to respond to biofeedback-identified and -strengthened signals.
5) What
degree of improvement is typically seen in patients with SCI?
Brucker
estimates that 98% of individuals with SCI who undergo his method improve
at least one vertebra level of functionality; therefore the condition of
an individual with cervical C7 SCI might improve to that generally found
in those with thoracic T1 injury. Nine-five percent of his patients
improve two vertebra functional levels, and 85% improve three.
Improvements greater than this are too erratic to predict. However,
biofeedback improvements may occur in functions controlled by nerves that
leave the cord far below the subject’s lesion, before being seen in
functions controlled by nerves that exit the cord just below the injury
site.
Depending on
which muscles can be fired through biofeedback and strengthened through
rehabilitation, it may be possible for previously wheelchair-using
individuals to stand and ambulate. Specific muscles (quadriceps) are
needed to stand, and others (hip flexors) are needed to walk. However, the
use of braces or adjusted patterns of gait might allow a subject to stand
or ambulate – even if control of the quadriceps and hip flexors is not
achieved. This also applies to the muscles of the calves, feet, and
ankles, or to the upper extremities. In other words, a BFB-trained
therapist will try to improve as many functions as possible. But if some
motor functions do improve, while others do not, improvements in limb
function might still be gained.
6) How
long does a typical session last for a subject with SCI?
One hour.
7) Has
biofeedback led to positive effects in SCI patients for urinary, bowel,
respiratory, spasticity/clonus, or pain issues?
Biofeedback can
produce positive effects on urinary incontinence, bowel control,
respiration, spasticity, and clonus. It is ineffective for treating
SCI-related chronic pain. Improved muscle tone and control of abdominal
muscles can indirectly improve bowel and bladder control. Spasticity and
clonus often decrease when improvements are made in voluntary motor signal
strength. Previously ventilator-dependant subjects have improved the use
of intercostal muscles, which assists breathing with the upper chest
cavity (as opposed to diaphragmatic breathing), allowing these individuals
to become ventilator independent.
8) How
many sessions are usually required to achieve maximum results?
Fifteen
sessions are normally advised for a course of biofeedback treatment for
SCI.
9) What
physical factors determine the outcome of biofeedback treatments?
To
be effective, neural pathways must be exist between the brain and muscles
that control desired functions. Neural signals over these connections may
be weak or the connection may be dormant. But a pathway must exist for
biofeedback to exert an effect. Target muscles must be able to respond to
neural signals. Excessive atrophy and tendon contractures can prevent the
use of limbs, regardless whether a neural connection is found or
strengthened.
10) Can
Biofeedback reverse muscular atrophy?
Muscle mass may
be improved if biofeedback therapy leads to functional use. Moderate to
severe atrophy may require the use of therapeutic electrical stimulation
to rebuilt atrophied muscles along with biofeedback. However, an initial
biofeedback evaluation can reveal if nerve signals are present in
atrophied muscles that might lead to functional improvements once the
muscles are rebuilt.
11) Are
additional rehabilitation regimens recommended for biofeedback subjects?
Biofeedback is more effective when combined with other forms of
rehabilitation.
For reasons
discussed before, it is recommended that individuals considering
biofeedback attempt to maintain flexibility, bone density, and muscle
mass. If biofeedback therapy succeeds in identifying and strengthening
neural pathways, physical rehabilitation may optimize their functional
use.
12) Are
follow-up treatments indicated once improvements plateau?
Once
improvements plateau, further biofeedback therapy is unlikely to lead to
additional gains. However, because neural repairs in the damaged spinal
cord can slowly occur over time, periodic biofeedback evaluation may
reveal new potentials for functional improvements.
13) Has
biofeedback been used with other function-enhancing modalities or
reparative/regenerative interventions?
Biofeedback has been used successfully with therapeutic electrical
stimulation to maintain or restore muscle mass and standard physical
rehabilitation practices. Because biofeedback offers an effective means
for finding new neural connections and training the patient in their
functional use, it should synergistically enhance the potential benefits
accruing from the many function-restoring therapies emerging throughout
the world.
14) Is
Biofeedback ineffective for any functions commonly lost or impaired
through SCI?
Biofeedback is
ineffective for restoring sensation lost through SCI. Nor does it
alleviate chronic pain due to spinal cord damage.
15) What
contraindications exist for biofeedback?
Because
biofeedback therapy does not “do” anything to the body, few
contraindications exist. However, because resulting functional
improvements can require strenuous physical effort, individuals interested
in biofeedback may need to be aerobically fit.
16)
Where is
the Brucker biofeedback method offered?
The procedure
is available in several locations in the U.S., Europe, the Middle East,
Central America, South America, and Asia (see below).
Conclusion:
In
conclusion, Brucker emphasizes: “Many individuals facing permanent
functional losses due to central nervous system (CNS) damage have
neurological potential for greater functional recovery, even long term
post onset. Biofeedback techniques can be extremely powerful in gaining
this increase in function through more efficient use of the CNS, but only
if applied properly.”
In addition
to improving the lives of individuals with SCI, Brucker believes that
biofeedback offers a valuable means for maximizing functional gains from
neural repairs – whether they occur naturally, or result from clinical
treatments. He notes: “Recent findings in neurological and behavioral
sciences have shown that CNS cells, if damaged, have potential for
remyelination and axonal repair which can take place years post damage
from injury or disease. It is also now known that the CNS can have both
dendrite and axonal sprouting in its attempt to regain integrity. While
the functional correlates of such neural repair were once thought to be
automatic, it is becoming clear that to maximize this neural potential,
specific learning techniques at the neuronal level are necessary. Advanced
biofeedback is the technique best suited for maximizing this potential.”