1) Antibiotics
2) Urinary Antiseptics
3) Bacterial
Interference
4) Nutritional
5) Alternative
Urinary-tract infections (UTIs) are an aggravating,
recurring health problem for individuals with SCI. According to the US
Agency for Health Care Policy and Research, 80% of those with SCI will
experience UTIs within 16 years of injury. UTIs are the most frequent
secondary medical complication during acute care and rehabilitation, and
urinary-system disorders are the fifth most common primary or secondary
cause of death. Waites and colleagues (Alabama, USA) estimated that the
incidence of UTIs with fever and chills in people with SCI was 1.82
episodes annually.
In the general population, most UTIs are caused by
Escherichia coli bacteria, which, although a normal part of our
intestinal miroflora, do not belong in our urinary system. In the case
of SCI, a diversity of bacteria can cause UTIs, including, in addition
to E. Coli, Klebsiella, Pseudomonas, Proteus,
Serratia, Providencia, Enterococcus, and
Staphylococcus.
Antibiotics
For more than 60 years, people with SCI have
relied on antibiotics to control UTIs. The development of these drugs
stems back to 1928 when British microbiologist and eventual Nobel
Laureate Alexander Fleming
 observed that bacterial growth was inhibited
by a penicillin-producing mold. Although infection-fighting molds have
been a part of mankind’s healing armamentarium since antiquity and noted
by scientists before Fleming, penicillin became the first antibiotic
isolated from one. The exigencies of World War II resulted in
penicillin’s production in sufficient quantities for general use. Since
then, scientists have developed many potent antibiotics.
observed that bacterial growth was inhibited
by a penicillin-producing mold. Although infection-fighting molds have
been a part of mankind’s healing armamentarium since antiquity and noted
by scientists before Fleming, penicillin became the first antibiotic
isolated from one. The exigencies of World War II resulted in
penicillin’s production in sufficient quantities for general use. Since
then, scientists have developed many potent antibiotics.
Although greatly increasing life expectancy for
people with SCI, the growth of antibiotic-resistant bacteria is of great
concern for this population that relies on their use. For example,
studies have shown every year two-million hospital patients acquire
infections that that they did not have when they entered the hospital;
of these, 80,000 die. Statistics such as these are especially relevant
to infection- and hospitalization-prone individuals with SCI and clearly
indicate the need to maintain antibiotic effectiveness.
In spite of commonly held assumptions that bacteria
are the bad guys, optimal health requires that we maintain a symbiotic,
health-enhancing partnership with them. For example, many different
bacteria living within our digestive system are essential for proper
digestion, nutrition, and long-term health. Every time we use an antibiotic, we undercut this
bacterial partnership. By constantly killing off the good guys as
collateral damage, we create a void that may be filled by
health-compromising pathogens or antibiotic-resistant bacteria that now
have no competition for growth.
In spite of their clear importance, every time you
use antibiotics you short-circuit your body’s inherent healing
potential, cumulatively compromising your long-term health. You may be
winning the immediate health-care battle, but you are setting yourself
up to lose the war.
In general, experts believe that antibiotics should
be reserved for the treatment of symptomatic UTIs and not
prophylactically used for prevention or treating asymptomatic
bacteriuria (i.e., bacteria in the urine without
symptoms). To minimize some of the antibiotic problems, the
chosen antibiotic should be tailored to the patient’s specific UTI
bacterial profile as determined by culture, and preferably a single
antibiotic should be used. Many antibiotics have been used to treat
SCI-associated UTIs, including cotrimoxazole, trimethroprim, mecillinam,
amoxicillin, norfloxacin, ciprofloxacin, cephalosporins, fosfomycin,
ceftazidine, meropenem, and piperacillin.

Urinary Antiseptics -
Methenamine
Used by many with SCI to combat UTIs, methenamine
derivatives (e.g., Hiprex®)
are urinary antiseptics that kill bacteria.
 Because
methenamine is not an antibiotic, bacterial resistance is not an issue.
If the urine is sufficiently acidic, the methenamine splits into ammonia
and bacteriostatic formaldehyde. Differences in acidification procedures
and, in turn, the amount of bacteria-killing formaldehyde that is
produced might explain some of the disparity in study results.
Because
methenamine is not an antibiotic, bacterial resistance is not an issue.
If the urine is sufficiently acidic, the methenamine splits into ammonia
and bacteriostatic formaldehyde. Differences in acidification procedures
and, in turn, the amount of bacteria-killing formaldehyde that is
produced might explain some of the disparity in study results.
Kevorkian and colleagues (Minnesota, USA) evaluated
methenamine’s UTI-preventing potential in 39 patients with a neurogenic
bladder (i.e., a malfunctioning bladder due to neurologic dysfunction)
who were in a program of intermittent catheterization and bladder
retraining. Twenty-two were male and 17 female, and age ranged
from 17 to 78 (average 30) years. Subjects received six 1-gram doses of methenamine daily or placebo for 21 days. Compared to an 86% infection
rate in placebo subjects, only 53% of the methenamine-treated patients
became infected.
Krebs and associates (Texas, USA) randomized 40 men
injured within the preceding half year to either methenamine-treated
(four 2-gram doses daily) or control groups.
After approximately 70 days, UTI incidence was significantly less in the
methenamine group. Specifically, the methenamine and control subjects
had 4 and 11 symptomatic UTIs, respectively.
Recently, Lee et al (Australia) looked at
methenamine’s UTI-fighting potential in 75 patients with SCI (Spinal
Cord 2007; 45).
Ranging in age from 16 to 82 (average 43.5) years, 83% were men and 55%
had cervical injuries. The average time since injury was 12 years.
Subjects consumed a daily one-gram methenamine dose for six months and
were compared to those who consumed a placebo or methenamine together
with cranberry (discussed below). No UTI-preventative effect could be
statistically documented for this treatment regimen. However, this study
used a much lower methenamine dosage than the previously discussed
investigations and did not ensure the urinary acidity supposedly
required for formaldehyde bacteriostatic release.
Bacterial
Interference
With the bacterial interference UTI-fighting
approach, innocuous bacteria are allowed to colonize the bladder, which,
in turn, inhibits colonization by the bad bacteria. Of course, any
antibiotic treatment during colonization would kill off the protective
bacteria. Studies focused on this topic have been carried out by
investigators, including Dr. Rabih
Darouiche, at research institutions in Houston, Texas (USA).

As reported in 2000, these investigators studied
the UTI-preventing potential of bacterial interference in 22 subjects
with SCI. All but three were men, age ranged from 32 to 55
years, and the time lapsing from injury varied from 5 to 24 months.
Subjects were inoculated in the bladder using a catheter with a benign
E. coli strain. Long-term bladder colonization with this
strain - lasting from 2 to 40 months - was achieved in 13 subjects.
Although these subjects had averaged 3.1 symptomatic UTIs annually
before colonization, no infections were observed after colonization as
long as the colonization remained in place. In contrast, infections were
observed in patients who were not successfully colonized and also in
those who lost colonization.
The next year, the investigators reported the
results of a larger study involving 44 subjects with SCI. Of the 44 inoculated with the same E. coli
strain mentioned above, 30 became colonized and experienced while
colonized a 63-fold reduction in symptomatic-UTI incidence compared to
their pre-study infection rate.
In 2005, the investigative team reported the
results of a rigorously designed prospective, randomized
placebo-controlled, double-blind pilot trial .
Of the 21 patients whose bladders were inoculated with the benign E.
coli strain, all were men, average age was 52, and 10 and 11 had
quadriplegia and paraplegia, respectively. Control subjects were
inoculated with a sterile saline solution. The investigators concluded
that colonized subjects were half as likely as non-colonized patients to
acquire a UTI during the following year.
In a much larger randomized, double-blind,
placebo-controlled study scheduled for completion in 2008, 160 patients
with SCI or spina bifida will be recruited from five medical centers in
Texas, Georgia, and Illinois. Because only about 1/3rd of
colonized subjects are expected to remain colonized for the 12-month
study period, subjects will be randomized in a 3:1 ratio. All subjects
will be treated with antibiotics before inoculation to eliminate
preexisting bacteria, and several days afterwards will be inoculated
with the protective E. coli strain or placebo.
The investigators have also studied bacterial
interference’s potential to reduce catheter-associated UTIs.
Bacterial biofilm that grows on implanted catheters can seed infections
on an on-going basis. The investigators concluded that pre-exposure of
the catheter to benign E. coli significantly reduced catheter
colonization by UTI-causing bacteria.
A 2009 study evaluated 13 individuals with SCI who
underwent 19 insertions of urinary catheters that had been
pre-inoculated with the benign E. coli strain. The catheter was
left in for three days and then removed. Of these individuals, eight
became successfully colonized with the benign strain. Before this
intervention, these individuals averaged 2.27 UTIs per year, afterwards
only 0.77 UTIs per year.
Nutritional Approaches
Cranberries: Cranberry products are a
traditional UTI-fighting folk remedy embraced by the SCI community. In
addition to supposedly acidifying the urine, cranberries contain
substances that inhibit bacteria from attaching to the bladder lining
and, as such, flush out bacteria with the urine stream.

Pilot-study results involving 15 subjects with SCI
carried out by Dr. Gregor Reid
and colleagues (Canada) suggested that
drinking cranberry juice greatly reduced bacterial attachment to
cells lining the bladder. Promisingly, this was a broad-spectrum, anti-bacterial
effect not limited to merely E. coli, the UTI-causing culprit in
the general population.
In 2008, Dr.
Marika Hess and colleagues (USA) reported the results of
randomizing 47 subjects with SCI to receive either cranberry extract
tablets or placebo. After six months, the treatments were reversed;
i.e., the placebo-treated subjects now received cranberry tablets, and
the cranberry-treated subjects now received placebo. On average, the
cranberry-treated subjects had only 0.3 UTIs per year compared to 1.0
UTIs of placebo-treated subjects. The investigators concluded that
“cranberry extract tablets should be considered for the prevention of
UTI in SCI patients with neurogenic bladder.”
However, the UTI-fighting properties of
cranberry-containing supplements (i.e., extracts not juice) could not be
demonstrated in several other studies.
For example, Dr.
Todd Linsenmeyer et al (USA)
randomized 21 subjects to receive either a cranberry tablet or inactive
placebo for four weeks.
 After a one-week washout period, the subjects who had received the
cranberry supplement were now given the placebo and vice versa. No
statistical difference was noted between the placebo and cranberry
groups as measured by several UTI-indicative criteria. Furthermore,
urinary acidity did not differ between the treatment groups.
After a one-week washout period, the subjects who had received the
cranberry supplement were now given the placebo and vice versa. No
statistical difference was noted between the placebo and cranberry
groups as measured by several UTI-indicative criteria. Furthermore,
urinary acidity did not differ between the treatment groups.
In another example,
Dr. K. B. Waites
and colleagues (USA)
compared 26 subjects with SCI who received a two-gram daily dose of
cranberry extract in capsule form for six months with 22 placebo-treated
subjects. The investigators concluded that the cranberry
extract did not reduce UTIs.
Dr. B. B. Lee
and associates
(Australia) evaluated the effects of cranberry tablets in preventing
UTIs in 78 subjects with SCI.
Subjects consumed an 800-milligram dose of cranberry twice daily for six
months. No difference in UTI incidence was noted between cranberry and
placebo-treated groups.
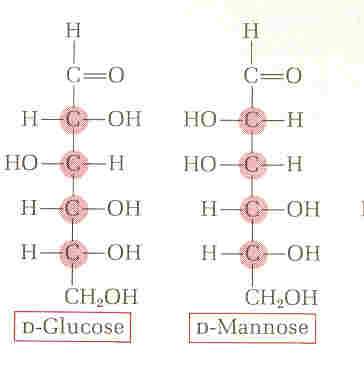
D-Mannose: Evidence indicates that D-mannose
is effective in dislodging E. coli bacteria from the bladder
wall, and, as can ameliorate many of the UTIs caused by this bacteria,
including in individuals with SCI. D-mannose is a naturally occurring
sugar similar in structure to glucose (a component of table sugar).
 Because
the body metabolizes only small amounts of D-mannose and excretes the
rest in the urine, it doesn’t interfere with blood-sugar regulation,
even in diabetics.
Because
the body metabolizes only small amounts of D-mannose and excretes the
rest in the urine, it doesn’t interfere with blood-sugar regulation,
even in diabetics.
The cell wall of the UTI-causing E. coli has
tiny finger-like projections that contain complex molecules called
lectins on their surfaces. These lectins are cellular glue that binds
the bacteria to the bladder wall so they cannot be readily rinsed out by
urination. However, because D-mannose molecules will glom on to these
lectins and fill up all of the bacterial anchoring sites, the bacteria
can no longer attach to the bladder wall and are, therefore, flushed
away. In other words, unlike antibiotics, D-mannose does not kill any
bacteria, whether they are good or bad, but simply helps to displace
them.
Vitamin C:
Dietary supplementation with vitamin C is believed by many to inhibit
UTIs by increasing urine acidity. Based on this belief, Dr. Nils
Hjeltnes and colleagues (Norway) have initiated a study that will
evaluate vitamin-C’s UTI-fighting potential for SCI. Forty individuals
with SCI, who have had three or more UTIs over the previous two years,
will be randomized to receive one gram of vitamin C daily or no vitamin
C for one year, and the number of UTIs between groups will be compared.
Alternative Approaches
Herbal Medicine: Before modern medicine
started emphasizing chemically synthesized drugs, herbal remedies were
the cornerstone of most of the world’s healing traditions and even
today, are used by 80% of the world’s population who cannot afford
Western pharmaceutics. As concerns grow about drug side effects or
bacterial resistance, many are once again turning to herbal remedies to
treat diverse ailments, including UTIs.
Many urinary-system herbal remedies have a long
history of use by both Western and indigenous (e.g., Native American)
cultures; have been listed in numerous official medical resources before
our focus on synthesized drugs pushed them to the sidelines; and even
today, have been often sanctioned by European governments in efforts to
reconcile and integrate herbal and modern medicine perspectives.
Although little focus has been on the use of these
herbal remedies to treat SCI-specific UTIs, many of these remedies act
against E. coli bacteria, the primary UTI culprit in the general
and SCI population. Several UTI-fighting herbal remedies or medicinal
foods are listed below: